Inflammatory bowel disease (IBD) affects 1.6 million Americans1, with as many as 70,000 new diagnoses each year. The cause is relatively unknown, though it is certainly related to an immune system deficiency. There are two conditions that are included in the IBD diagnosis; Crohn’s Disease and Ulcerative Colitis. Each condition impacts the body in different ways, and both can be treated by a well-trained pelvic rehabilitation practitioner. Andrea Wood, PT, DPT, WCS, PRPC explains more in her recent post on The Pelvic Rehab Report.

A colon affected by ulcerative colitis
What are the symptoms of Inflammatory Bowel Disease?
According to Dr. Wood, “common complications experienced by patients with IBD include fecal incontinence, fecal urgency, night time soiling, urinary incontinence, abdominal pain, hip and core weakness, pelvic pain, fatigue, osteoporosis, and sarcopenia.”
What is the difference between Crohn’s Disease and Ulcerative Colitis?
While either condition is considered Inflammatory Bowel Disease, there are some differences between the two. Ulcerative Colitis affects the innermost lining of the colon exclusively, and it produces internal ulcers and open sores. Patients with Ulcerative Colitis will have inflammation and tissue damage throughout the inner lining of the colon.
Crohn’s Disease is a chronic inflammation anywhere in the digestive tract, though it most commonly impacts the bowel and colon. The bowel wall will be affected, and patients may experience patches of inflamed intestine interspersed with healthy areas of the intestine.
Both conditions can be life-altering for patients who suffer from them.
Can Inflammatory Bowel Disease be treated?
The cause of IBD may not be known, but the symptoms certainly are. A skilled pelvic rehabilitation practitioner, like a Pelvic Floor Physical Therapist, can help patients overcome symptoms like fecal incontinence, urinary urgency, sarcopenia, fatigue, or pelvic pain. According to Dr. Wood, these are some of the treatments that an IBD patient might be offered in her clinic:
| Fecal Incontinence | – Identify primary cause – Apply manual therapy – Biofeedback training to improve rectal pelvic floor muscle endurance and strength – Instruct in proper toileting posture and techniques – Rectal balloon training to better understand fecal urgency |
| Urinary Incontinence | – Urge suppression techniques – Bladder diaries and voiding intervals – Decrease usage of bladder irritants |
| Sarcopenia | – Weight training – Abdominal training that doesn’t increase intra-abdominal pressure |
| Fatigue | – Short bursts of cardiovascular exercise – Training in proper bowel movement timing to improve sleep – Diet and nutrition recommendations to improve sleep |
| Pelvic Pain | – Manual therapy externally and internally if needed – Home yoga program instruction – Meditation instruction |
Where can I find help?
Our directory of pelvic rehabilitation professionals can help you find a pelvic floor specialist today. Visit www.pelvicrehab.com to find a pelvic health practitioner near you, and get treatment for conditions like Inflammatory Bowel Disease.
1. Crohn’s and Colitis Foundation. 2019. What is Crohn’s Disease. Retrieved from: http://www.crohnscolitisfoundation.org/what-are-crohns-and-colitis/what-is-crohns-disease/
 Often colloquially called “mummy tummy”, “baby belly”, etc, diastasis recti abdominis occurs when the abdominal muscles are separated vertically, along what’s called the linea albia. Clinically you would be diagnosed with diastasis recti if you have more than 2cm of separation while doing a hook lying curl exercise.
Often colloquially called “mummy tummy”, “baby belly”, etc, diastasis recti abdominis occurs when the abdominal muscles are separated vertically, along what’s called the linea albia. Clinically you would be diagnosed with diastasis recti if you have more than 2cm of separation while doing a hook lying curl exercise. 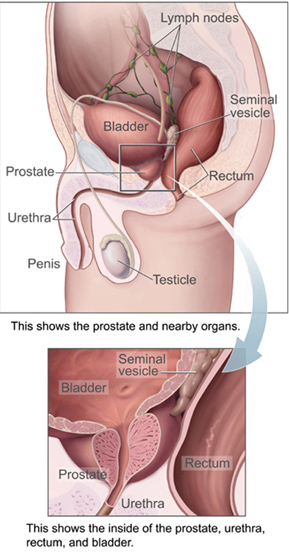 One big problem is that different conditions can express themselves in similar ways. Prostatitis can cause sexual dysfunction, difficult and painful urination, pain in the perineum, testicles, bladder, and penis. These symptoms may also be caused by a number of other conditions as well. Chronic Pelvic Pain Syndrome can be caused by muscle spasms. Bladder malfunction can be caused by interstitial cystitis. Erectile dysfunction may be related to hormone or testosterone imbalances.
One big problem is that different conditions can express themselves in similar ways. Prostatitis can cause sexual dysfunction, difficult and painful urination, pain in the perineum, testicles, bladder, and penis. These symptoms may also be caused by a number of other conditions as well. Chronic Pelvic Pain Syndrome can be caused by muscle spasms. Bladder malfunction can be caused by interstitial cystitis. Erectile dysfunction may be related to hormone or testosterone imbalances.